
Many have assumed that densely populated areas like city centers are more conducive to the spread of COVID-19. A new study, published in the Journal of the American Planning Association, finds that the opposite may be true. Researchers from the University of Utah and the Johns Hopkins Bloomberg School of Public Health examined both infection and death rates in 913 U.S. metropolitan counties and found that population size, not density, corresponded to mortality rates. One possible explanation could be faster and more widespread adoption of social distancing practices and better quality of health care in areas of denser population.
“Our findings run counter to the recent narrative about escaping compact cities for sprawling suburbs as a way of staying safe from COVID-19,” said co-author Reid Ewing, distinguished professor in the Department of City & Metropolitan Planning at the University of Utah. “This is one more reason for urban planners and public officials to favor compact urban development over suburban sprawl. Compact places seem to promote better adherence to social distancing and provide better acute health care, so those contracting the coronavirus are less likely to die.”
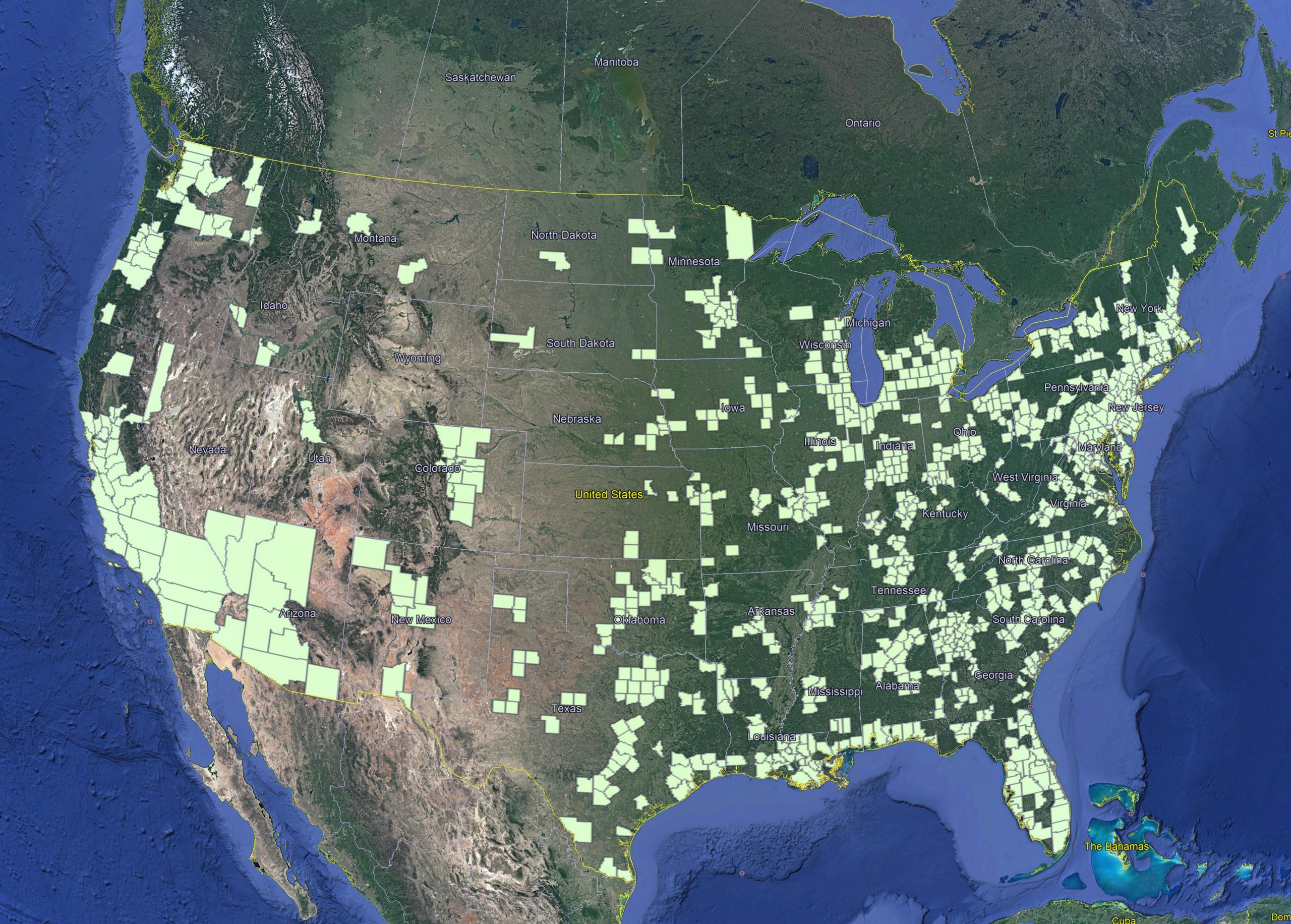
A map of the 913 U.S. metropolitan counties included in the survey.
The three-member team chose to examine county data, not individual cities, between Jan. 20-May 25, 2020. Large cities alone have multiple unknown variables. Counties, on the other hand, have multiple known factors that allowed the team to find the “activity density” of each and make comparisons. Activity density = (population of a county + jobs in the county)/area of the county.
Activity density takes into account both the county residents and workers commuting within a given area. Other factors, such as population size, education levels, and demographic variables, including age and race and health care infrastructure (ICU bed capacity), were also considered.
“Our analysis shows that metropolitan size is more important than density,” said co-author Sadegh Sabouri, doctoral student in the Department of City & Metropolitan Planning at the U. “Take Dutchess County, New York, for example, being surrounded by one of the largest metropolitan areas—New York, Newark and New Jersey City. The activity density is 518.1 and death rate of 4.63 per 10,000. Salt Lake County, by comparison, is located in a metropolitan area that is one-twentieth the population and has a density four times higher at 2060.2 and a death rate of only 0.61.”
The analysis did not indicate a significant association with infection rates. However, higher activity density did have a significant and unexpected association with death rates. They found that after controlling for factors such as metropolitan size, education, race and age, doubling the activity density was associated with an 11.3% lower death rate.
They also conclude that counties with higher proportions of people ages 60 and older, lower proportions of college-educated people, and higher proportions of African Americans experienced greater infection and mortality rates.
The researchers have been updating the data as the pandemic has progressed and are finding that the associations uncovered in their study are becoming even stronger. The team is also conducting a longitudinal study that tracks the relationships among county density, infection and mortality rates and explanatory factors as they change over time. They have found consistent results regarding the inverse relationship between density and the COVID-19 mortality rate.
Find the full study here.